Over the past 10 years, a growing body of research in immunology and cancer biology has led to an enhanced knowledge of the complex interactions between cancer and the immune system. This complex relationship can be described by the hypothesis of cancer immunoediting, which encompasses the dynamic of tumor development over time. Figure 1 displays a brief overview of the 3 phases of immunoediting.
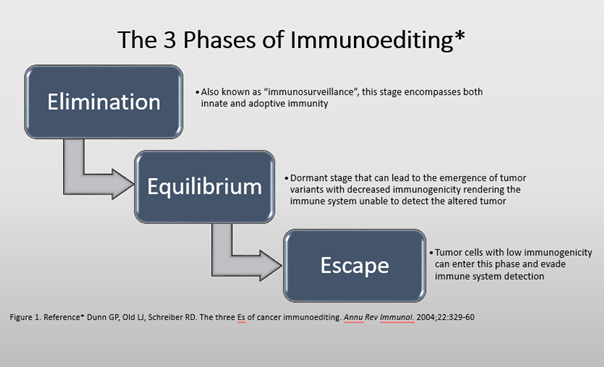
Figure 1: Phases of Immunoediting
CTLA-4 and PD-1 are inhibitory protein receptors found largely on the surface of effector T-cells. The ligand for PD-1, PD-L1, is broadly expressed on tumor cells either endogenously or via induction by association with T-cells (Figure 2). The difference between these receptors is the setting in which they act: CTLA-4 regulates T-cell activity at an early stage while PD-1 regulates effector T-cell activity within tissues and tumors.
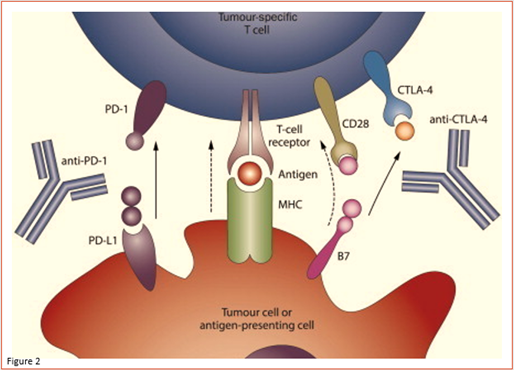
Figure 2: Immune “Checkpoint” Proteins in Cancer Cells
Immune checkpoints generally work as physiological “brakes” to prevent over-activation of T-cells and thus prevent cell-mediated autoimmunity. For example, binding of PD-L1 to PD1 leads to inhibition of intracellular signaling pathways controlling T cell activation. PD-1/PD-L1 interaction results in T cell suppression possibly via several mechanisms (anergy, exhaustion, and death). It has thus been postulated that blocking the PD-1/PD-L1 interaction with monoclonal antibodies directed to either PD-1 or PD-L1 leads to inhibition of the PD1/PD-L1 signaling pathway, re-activation of T lymphocytes, and stronger anti-neoplastic responses. Several other proteins aside from CTLA-4 and PD-1/PD-L1 that play a role in crucial steps of the cell immune cycle have been considered as potential targets for immunotherapies. These includes CD137, OX40 and CD27 (priming and activation), vascular endothelial growth factor (infiltration of T-cell into tumors), Toll-like receptors, and CD40 (antigen presentation).
References
- Dunn GP, Old LJ, Schreiber RD. The three Es of cancer immunoediting. Annu Rev Immunol. 2004;22:329-60.
- Garon EB. Current Perspectives in Immunotherapy for Non-Small Cell Lung Cancer. Semin Oncol. 2015;42(Suppl 2):S11-S18.
- Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer.2012;12(4):252-64.
- Topalian SL, Hodi FS, Brahmer JR, et al. Safety, Activity, and Immune Correlates of Anti-PD-1 Antibody in Cancer. N Engl J Med. 2012;366(26):2443-54.
- Taube J, Anders R, Young G, et al. Colocalization of inflammatory response with B7-H1 expression in human melanocytic lesions supports an adaptive resistance mechanism of immune escape. Sci Transl Med. 2012;4(127):127-137.
- Intlekofer AM, Thompson CB. At the bench: preclinical rationale for CTLA-4 and PD-1 blockade as cancer immunotherapy. J Leukoc Biol. 2013;94(1):25-39.
- Kim JM, Chen DS. Immune escape to PD-L1/PD-1 blockade: seven steps to success (or failure). Ann Oncol. 2016;27(8):1492-504